Congenital Zika Syndrome
A distinct pattern of other birth defects, called congenital Zika syndrome, has been found. Congenital Zika syndrome is unique to fetuses and infants infected with Zika virus before birth, and is described by the following five features:
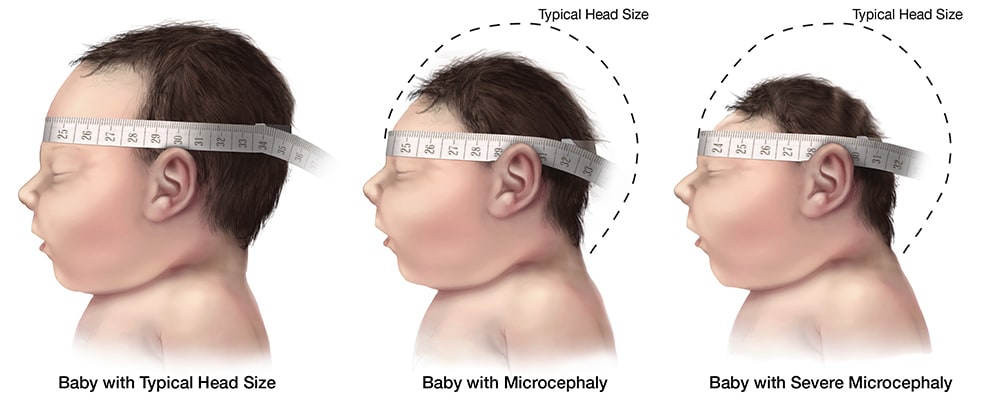
- Severe microcephaly in which the skull has partially collapsed
- Decreased brain tissue with a specific pattern of brain damage, including subcortical calcifications
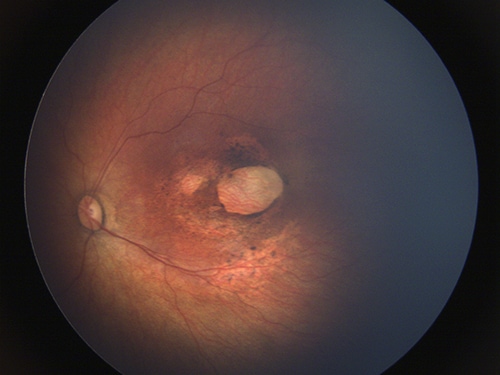
- Damage to the back of the eye, including macular scarring and focal pigmentary retinal mottling
- Congenital contractures, such as clubfoot or arthrogryposis
- Hypertonia restricting body movement soon after birth
Congenital Zika virus infection has also been associated with other abnormalities, including but not limited to brain atrophy and asymmetry, abnormally formed or absent brain structures, hydrocephalus, and neuronal migration disorders. Other anomalies include excessive and redundant scalp skin. Reported neurologic findings include, hyperreflexia, irritability, tremors, seizures, brainstem dysfunction, and dysphagia. Reported eye abnormalities include, but are not limited to, focal pigmentary mottling and chorioretinal atrophy in the macula, optic nerve hypoplasia, cupping, and atrophy, other retinal lesions, iris colobomas, congenital glaucoma, microphthalmia, lens subluxation, cataracts, and intraocular calcifications.
Microcephaly
Microcephaly is a congenital malformation resulting in smaller than normal head size for age and sex. It has also been associated with other birth defects and neurologic conditions in children and adults. For infants diagnosed with microcephaly, head size correlates with underlying brain size. However, these measurements do not consistently predict long term sequelae. Neurologic sequelae may include seizures, vision or hearing problems, and developmental disabilities. Symptoms vary with the extent of brain disruption.
There is now scientific consensus that Zika virus infection during pregnancy is a cause of microcephaly. We do not know if a newborn who gets Zika virus infection around the time of birth will develop microcephaly after birth. Babies can develop microcephaly after birth if their head growth slows or fails to develop. There have been no reports of Zika virus infection around the time of birth leading to microcephaly in infants.

Diagnosis of Microcephaly
Microcephaly is diagnosed when an infant’s head is smaller than expected as compared to infants of the same age (or gestational age) and sex. For the purpose of evaluating an infant for possible congenital Zika virus infection, microcephaly is defined as occipitofrontal circumference less than the third percentile, based on standard growth charts for sex, age, and gestational age at birth. For a diagnosis of microcephaly to be made, the occipitofrontal circumference should be disproportionately small in comparison with the length of the infant and not explained by other etiologies (e.g., other congenital disorders).
INTERGROWTH-21st Fetal Growth Standards are based on measurements in utero only. International standards for birth measurements in infants less than 24 weeks gestation are not available. For most elective pregnancy terminations and many stillbirths, accurate postnatal head circumference measurements are not possible.
For a study comparing head circumference measurements in utero to those obtained after birth, see: Melamed N, Yogev Y, Danon D, et al. Sonographic estimation of fetal head circumference: how accurate are we? Ultrasound Obstet Gynecol 2011;37:65-71.
In the setting of Zika virus infection, the head circumference might be disproportionately small in comparison with the length of the infant and not explained by other etiologies.
Measuring Head Circumference
Head circumference (occipitofrontal circumference) measurements should be taken using a tape measure that cannot be stretched. The tape is securely wrapped around the widest possible circumference of the head, 1–2 finger widths above the eyebrow on the forehead and at the most prominent part of the back of the head. Ideally, the measurement should be taken 3 times and the largest measurement recorded to the nearest 0.1 cm. It may be helpful to have the parent or nurse hold the infant’s arms.
Although head circumference measurements may be influenced by molding and other factors related to delivery, the measurements should be taken on the first day of life because commonly-used birth head circumference reference charts by age and sex are based on measurements taken before 24 hours of age. The most important factor is that the head circumference is carefully measured and documented. If measurement within the first 24 hours of life is not done, the head circumference should be measured as soon as possible after birth.
Ocular Findings in Babies with Congenital Zika Virus Infection
Ocular abnormalities have been reported in infants with congenital Zika virus infection with and without microcephaly or other central nervous system anomalies. Ocular findings have been reported involving both the anterior and posterior parts of the eye. Among infants with presumed congenital Zika virus infection, the most commonly reported structural ocular abnormalities involve the macula and the optic nerve.
The most commonly reported macular findings include- Focal pigmentary mottling
- Chorioretinal atrophy
- Optic nerve hypoplasia
- Optic nerve cupping
- Optic nerve atrophy
Other ocular findings that have been reported in infants with congenital Zika virus infection include, but are not limited to
- Other retinal lesions: subretinal hemorrhage, hypopigmentation, vascular tortuosity, abnormal termination of the vessels, focal vascular dilation
- Congenital glaucoma
- Iris colobomas
- Microphthalmia
- Cataracts
- Subluxation of the lens
- Intraocular calcification
No comments:
Post a Comment